STEPS to Care: Care Plans
Comprehensive Care Plans help clients work with their Care Team to plan, document, and accomplish individualized care goals and healthier outcomes.
Care Plans are also used and reviewed in Care Team Coordination Meetings and medical appointments to ensure clients are keeping up with their health goals.
After reviewing the information and resources below, you will know:
- How Care Plans are used as part of STEPS to Care
- Who should create and update Care Plans
- How to work with clients to create effective Care Plans
Using a Comprehensive Care Plan with Clients
The Comprehensive Care Plan sets client goals, identifies activities or action steps needed to achieve these goals, expected dates for each action step, and any resources or support needed to complete the Care Plan. Each action step on the Care Plan should list a responsible party, target date, outcome, and outcome date. The plan also incorporates behavioral health, nursing, and other specialist and allied health professional plans as needed.
Comprehensive Care Plan
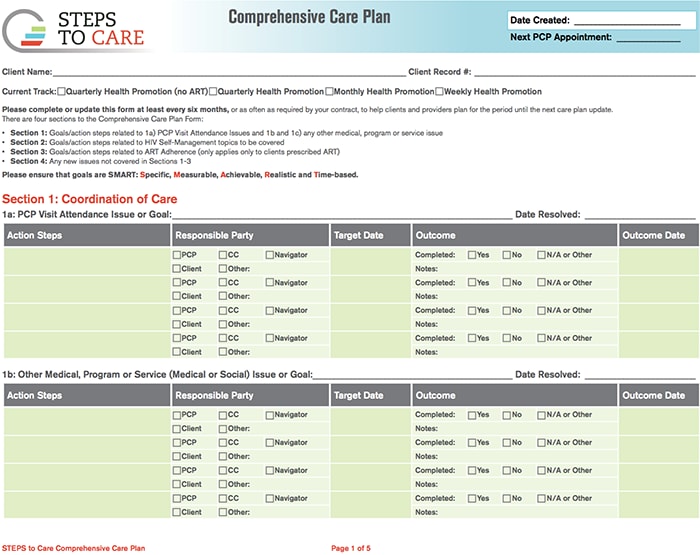
The Comprehensive Care Plan is a four-section written plan developed by the client’s medical provider, the Care Coordination Team and the client to help the client achieve his or her treatment goals.
See the SMART Goals training below to learn more about working with clients to create goals and action steps for the Care Plan.
[PDF - 499 KB]
Who Completes and Maintains the Care Plan?
- All Care Team members are involved in the Care Plan, but the Care Coordinator is primarily responsible for maintaining the plan regardless of which program staff completed it.
- The Patient Navigator is an active participant in the creation of the Care Plan, ensuring that it is client-centered and incorporates the client’s goals.
- All Care Team members providing care to the client participate in and contribute to the Care Plan during Care Team meetings.
- The Primary Care Provider reviews the Care Plan with the client at the end of every primary care visit. The Care Coordinator and/or Patient Navigator should also be part of this review.
- Any changes to the care plan are also reviewed at the next Care Team meeting. Patient Navigators can also make changes to the Care Plan after client navigation meetings with a client.
- Developing an effective Comprehensive Care Plan involves all Care Team members. This graphic explains the stages and cycle of the Comprehensive Care Plan and who is involved each step of the way.
